 Join the network
Join the network
Blog
Income generation and malaria in Uganda
Several large-scale efforts have been made to combat malaria in the last decade under the Millennium Development Goals, and while these have led to a rapid decline in cases, malaria continues to exact a heavy toll on sub-Saharan Africa, both in terms of human life and economic cost.
Given the relative importance of agriculture in sub-Saharan Africa, several papers have speculated on the possibility that the income-generating capacity of agriculture may help to reduce malaria. However, malaria and income share a complex two-way relationship, and identifying the direction of causality has been a challenge. On the one hand, malaria-related mortality and mobility can reduce income through lost earnings and reduced productivity. On the other hand, low income can increase incidence of malaria by reducing capacity to buy bed nets and other preventive measures. In Pan and Singhal (2015) we contribute to the literature by examining the effects of a large agricultural income-generating program on malaria in Uganda.
Malaria in Uganda
Malaria spreads through the bites of female mosquitoes that are infected with the malaria parasite. Malaria is endemic in Uganda and it suffers from one of the highest malaria incidence rates in the world (WHO 2015). The economic costs of a malaria episode are high — estimated to be approximately 7.2% of the average annual per capita non-health consumption expenditure of a household (Hoffmann et al. 2009). Sleeping under a bed net is one of the most common ways to prevent mosquito bites. Despite the efforts of the Uganda National Malaria Control Program (UMCP) to provide free or subsidized bed nets, poor households continue to face substantial financial hurdles in obtaining bed nets.
A program to improve agricultural productivity
BRAC Uganda, a large NGO, launched an agricultural extension services program in 2008 with the objective of increasing the productivity of small, low-income female farmers by encouraging them to adopt modern cultivation techniques. This was done by providing agricultural training and increasing access to inputs such as high-yield variety seeds. Within three years (2008-11), it is estimated that the program reached 64,000 farmers across 41 districts in Uganda. The program was found to be effective in increasing the adoption of techniques and inputs that require little upfront monetary investments — intercropping, crop-rotation, use of manure. This in turn improved food security of the households (Pan et al. 2015).
An important aspect of the program was that it was only limited to villages lying within a radius of six kilometers from BRAC branches. This rule was chosen by BRAC to balance the need to reach as many farmers as possible against transportation costs for program assistants. From the point of view of our study, this rule allows to casual identification of the effects of the program by comparing villages that lie just within the program boundary to those that lie just beyond the boundary.
The analysis is conducted using two datasets. First, we use a household survey conducted by BRAC Uganda in 2011, three years after the start of the intervention. In addition to several socioeconomic welfare indicators, the survey also asked each household member if they had suffered from malaria in the six months preceding the survey. The survey also collected GPS locations of the households that allow us to compute the distance of villages from the 6km boundary that defines program eligibility. Second, we also use the Uganda National Household Survey 2005-06 to verify that eligible and ineligible households look similar in the pre-intervention period.
How does access to the program affect malaria prevalence?
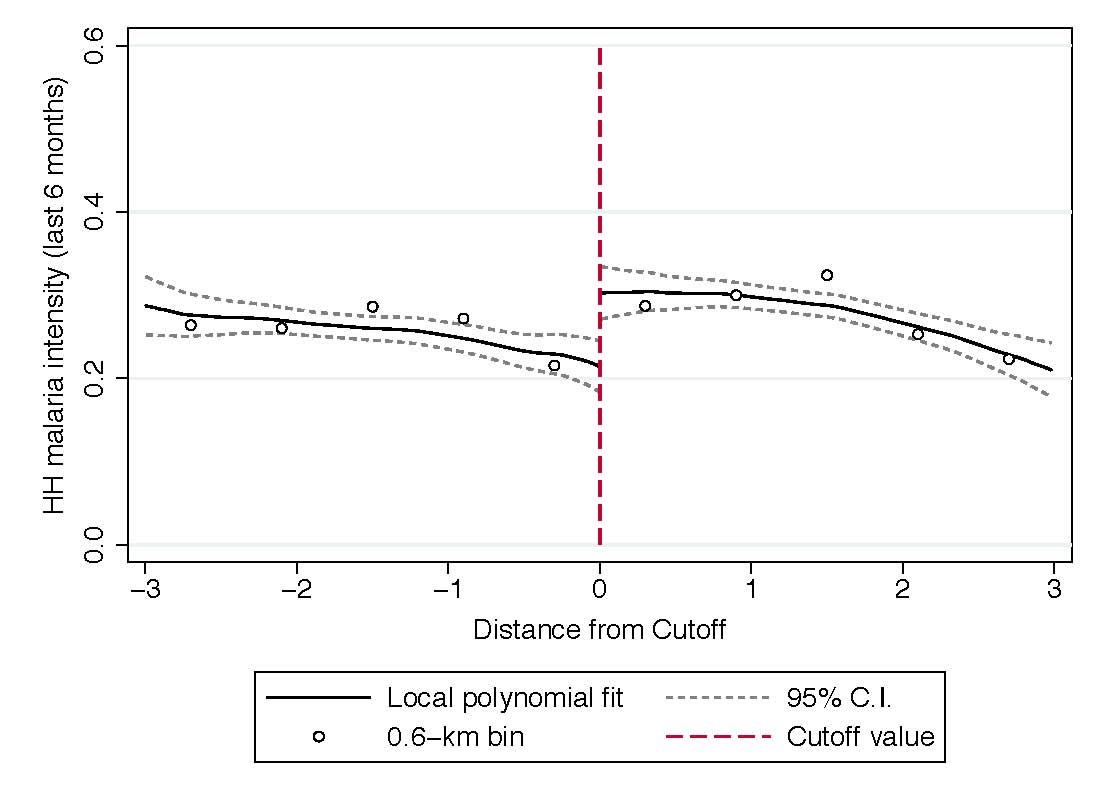
We find that access to the agricultural extension services program reduces malaria prevalence. This can be seen in Figure 1, where the y-axis depicts the proportion of household members who were infected by malaria in the preceding six months. The x-axis measures the distance of the village from the 6km boundary, depicted by 0 such that those to the left of 0 were eligible for the program and those on the right were ineligible. The results estimate that access to the program reduces proportion of household members affected by malaria by 8.9 percentage points (or 29% relative to the control average). While prevalence of malaria declines for all ages groups and genders, the effects are particularly large for those most vulnerable to malaria — children aged 5 or less, and pregnant women.
Figure 1: Access to the agricultural extension services program reduces malaria prevalence
An examination of the underlying mechanisms indicates that an increase in household income and the resulting increase in the ownership and usage of bed nets drives these effects. We find that the value of agricultural production per capita (proxy for income) increased by 27.5% due to the program. Correspondingly, the number of bed nets owned per capita increased by 22%. We were also able to rule out several alternative mechanisms such as differences in access to various forms of healthcare, health-related information, agricultural practices, female bargaining power, fertility, and mortality that could be affecting the results.
Substantial long-term benefits
We find that access to a large income-generating program led to a substantial decline in prevalence of malaria in Uganda. The effects are largely concentrated among the most vulnerable groups — children under the age of 5 and pregnant women. The explanation most consistent with our data seems to be that the reduction in malaria is driven by an increase in incomes, highlighting the importance of financial constraints in investments in preventive healthcare. As exposure to health shocks in early life can translate into considerable economic losses over time, our results imply that the agricultural extension services program could have substantial long-term benefits that are not accounted for in standard cost-benefit analyses.
References
Hoffmann, V., C.B. Barrett, and D.R. Just (2009). ‘Do free goods stick to poor households? Experimental evidence on insecticide treated bed nets’. World Development, 37(3): 607-617.
Pan, Y., and S. Singhal (2015). ‘Income and malaria: Evidence from an agricultural intervention in Uganda’. WIDER Working Paper, 92/2015. Helsinki: UNU-WIDER.
Pan, Y., S. Smith, and M. Sulaiman (2015). ‘Agricultural extension and technology adoption for food security: Evidence from Uganda’. IZA Discussion Paper No. 9206.
World Health Organization (WHO) (2015). World Malaria Report 2015. Geneva: World Health Organization.
The views expressed in this piece are those of the author(s), and do not necessarily reflect the views of the Institute or the United Nations University, nor the programme/project donors.

